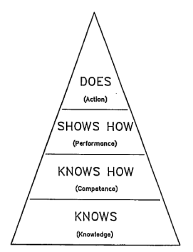
Simulation has filled a void that was once present in medical education. Written and oral examinations continue to be used to assess Miller’s “knows” and “knows how” levels of performance while clinical rotation evaluations rest at the top of the triangle: “Does”. Simulation completes Miller’s triangle by allowing learners to “show how” their knowledge and skills can be applied in a risk-free, simulated clinical environment. 1-2
As simulation educators, our roles not only include creating, programming, running realistic scenarios and facilitating debriefing, but also developing appropriate learning objectives that align with our instructional strategy of simulated team-based resuscitation.
Learning objectives are statements of what we intend or expect students to learn as a result of our instruction. In order to create these objectives, we need to determine what kind of knowledge and cognitive processes we are trying to address in our learners through the use of simulation. This is where learning theories can help.
Learning Objective Taxonomy
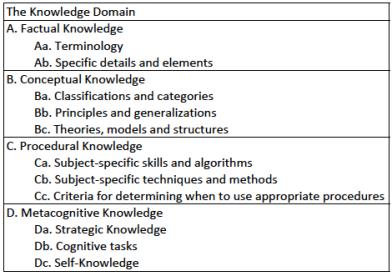
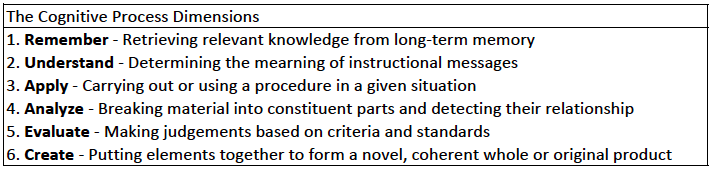
Bloom originally described a hierarchical taxonomy of educational objectives based on 6 categories of the cognitive domain from simple to more complex: Knowledge, Comprehension, Application, Analysis, Synthesis and Evaluation.3 In 2002, Krathwohl presented a revision of Bloom’s Taxonomy that expanded and described the different categories of knowledge in increasing complexity from factual to metacognitive knowledge. He also described a novel approach to educational objectives involving two dimensions: a combination of the type of knowledge and the cognitive process involved in obtaining that knowledge.
This combination represents the way learning objectives are usually developed and written; there is a component of subject content as the noun (the knowledge domain) and a description of what is to be done with that content as the learning verb (the cognitive process dimension).
An instructor can develop learning objectives for simulation that fall under any knowledge domain and cognitive process dimension but being a learning modality that can be limited by resources, cost, space and time, I believe that these learning objectives should be optimized to the most appropriate cognitive process dimension and should specifically target subject content from a complex knowledge domain so that learners get the most out of the simulated experience. Compare these 3 examples of learning objectives for a simulated scenario of unstable bradycardia.
Ex 1: Understand the treatment of a patient with unstable bradycardia.
Ex 2: Recall the appropriate dose of atropine in the setting of unstable bradycardia.
Ex 3: Appropriately employ the ACLS bradycardia algorithm to a patient in 3rd degree AV-block.
In example 1, the learning verb, to understand, is ill defined. A non-specific learning verb makes it more difficult to assess the learner’s performance. Also, while treatment as the noun may be classified as conceptual knowledge, it is too vague to tailor specific debriefing comments towards.
In example 2, the learning verb recall uses the lowest level of cognitive processes: remembering. Also, the dose of atropine represents factual knowledge, the lowest level of the knowledge domain. While this could be an objective for a simulated scenario, the objective could also be adequately (or even more appropriately) met using less complex instructional strategies (textbooks, blogs or lectures) or assessment tools (paper tests or oral exams).
In example 3, the learning verb employ targets the highest cognitive process dimension of the three examples: to apply. The ACLS bradycardia algorithm represents procedural knowledge that is well defined which helps both the learners and educators understand their expectations. The learning objective is specific and tailored to the case.
Which levels of knowledge and cognitive process dimensions should we target?
While learners in simulated scenarios do employ factual and conceptual knowledge in the evaluation, diagnosis and treatment of the simulated patient, I think the facets of procedural knowledge (remember, this is the educational theory “procedural”, not cricothyroidotomy “procedural”) best represent the kind of knowledge simulation can afford to learners. These facets include subject-specific skills, algorithms, techniques, methods and criteria for determining when to use appropriate procedures. Debriefing scenarios can also incorporate the metacognitive domain as learners can reflect on their performance and gaps in their knowledge. The apply dimension, which includes executing and implementing procedures in a given situation, most adequately describes the cognitive process used by learners during simulated scenarios while debriefing may involve evaluating certain processes.
Each cognitive domain process has useful learning verbs associated with them to help us create targeted learning objectives.

Final Tips
So, when developing your learning objectives for a simulated scenario, targeting a specific knowledge domain and cognitive process as the learning noun and verb, respectively, will help guide the process. To optimize the learning objective and align it with the instructional strategy of simulated resuscitation scenarios, try and aim for a more complex knowledge domain (such as procedural knowledge) and a higher cognitive process.
Now that we know some of the theory, what kind of objectives should we make? Should we focus on medical management? What about crisis-resource management? In part 2, we will tackle what kind of learning objectives should be included in a team-based resuscitation simulated scenario.
References
1) Miller, G. (1990). The assessment of clinical skills/competence/performance. Academic Medicine,65(9), S63-7.
2) Kyle, R. (2008). 7.5 Which of these Curriculum Components are Best Suited to Simulation? In Clinical simulation operations, engineering and management(1st ed., pp. 78-79). Burlington, MA: Academic Press.
3) Bloom, B.S., Engelhart, M.D., Furst, E.J., Hill, W.H., & Krathwohl, D.R. (1956). Taxonomy of educational objectives: The classification of educational goals. Handbook 1: Cognitive domain. New York: David McKay
4) Krathwohl, D. (2002). A Revision Of Bloom’s Taxonomy: An Overview. Theory Into Practice,41(4), 212-218.

2 thoughts on “How to develop targeted simulation learning objectives – Part 1: The Theory”