This case was written by Drs. Alexandra Stefan and Marissa Lu.
Dr. Stefan (@astefan12) is an emergency physician at Sunnybrook Health Sciences Centre and University Health Network, and assistant professor in the Division of Emergency Medicine, University of Toronto. She is the Co-Director of Postgraduate Education in the Sunnybrook Emergency Department. Her interests include physician wellness, medical education, global health education, and she has been faculty for several teaching trips with the Toronto Addis Ababa Academic Collaboration. She believes that simulation is valuable education tool for health care providers to develop and practice a broad range of clinical skills, from ACLS to goals of care discussions.
Dr. Lu is a PGY1 Emergency Medicine resident at the University of Toronto. Her interests include medical education (particularly in-situ simulation and pedagogy) and physician wellness. She completed her BSc (Psychology, Neuroscience and Behaviour) at McMaster and her MD at the University of Toronto.
WHY IT MATTERS
TB is an important cause of morbidity and mortality worldwide. While it is relatively rare to have TB present as tamponade secondary to pericarditis, it is a recognized complication that requires emergent management. It is important to think about and investigate for TB in any patient with risk factors and constitutional symptoms and this case provides a great opportunity to discuss this along with the emergency management of pericardial tamponade.
CLINICAL VIGNETTE
You are working in the acute area of the ED of a community hospital. You are called to assess a patient by the RN who is concerned about the patient’s respiratory status. You meet Mr. Tesfaye and his cousin; the patient is complaining of chest pain and severe shortness of breath.
CASE SUMMARY
A 38 year-old man (Ethiopian refugee) with untreated HIV and past history of TB, presents to the emergency department (ED) with anterior chest pain, shortness of breath and hypotension. He was seen 3 days prior by a walk-in clinic and referred to the ED with chest pain and ECG showing pericarditis, but did not attend the ED until symptoms were severe. In the ED, patient quickly progresses to profound shock and has a PEA arrest. POCUS will show a large pericardial effusion and tamponade. Team members are to initiate CPR, manage the arrest and treat the effusion using bedside pericardiocentesis in order to obtain return of spontaneous circulation (ROSC).
DOWNLOAD THE CASE HERE:
ECGs/CXR FOR THE CASE FOUND HERE:
ECG from walk in clinic:
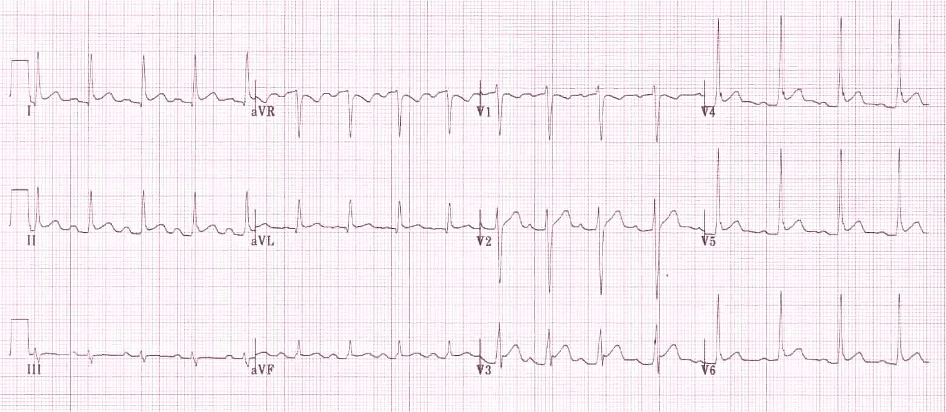
Source = https://lifeinthefastlane.com/ecg-library/basics/pericarditis/
ECG from ED:
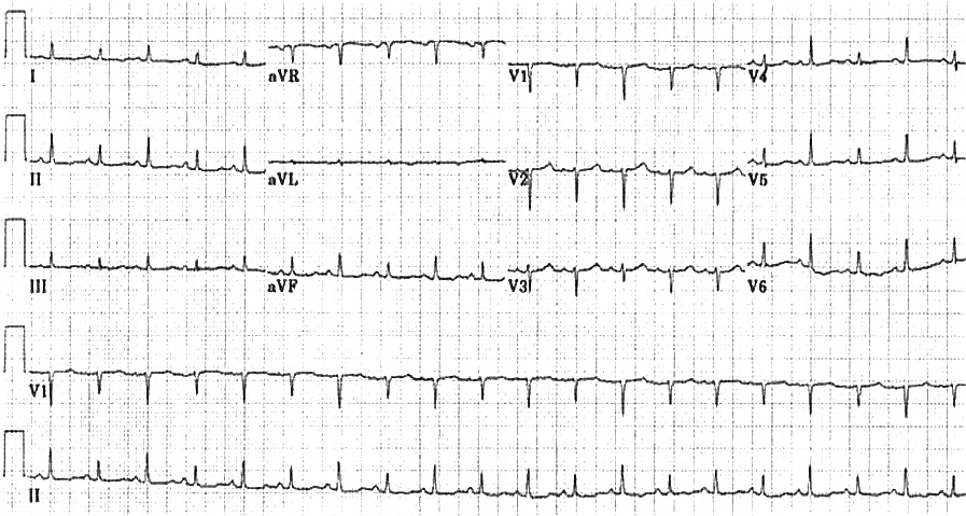
Source = https://lifeinthefastlane.com/ecg-library/electrical-alternans/

Source = https://radiopaedia.org/cases/pericardial-effusion-water-bottle-sign-2

This was a FANTASTIC case and the teaching points were spot on relevant and I think this case was expertly done!
LikeLike