This case was written by Dr. Martin Kuuskne who is one of the editors-in-chief at EMSimCases and is an attending Emergency Medicine Physician at University Health Network in Toronto.
Why it Matters
Aortic Dissection is one of the most deadly causes of chest pain for the emergency physician. Its presentation, methods of diagnosis, management and complications are varied and demand critical thinking, clear communication and teamwork. This case highlights the following points:
- The key elements of the history, physical exam and initial investigations that support the diagnosis of aortic dissection.
- The importance of managing hypertension in the setting of aortic dissection, including specific blood pressure and heart rate targets.
- The need to set priorities dynamically as a patient becomes unstable and requires ACLS care.
Clinical Vignette
You are working the day shift at a tertiary-care hospital. A 66-year-old female is being wheeled into the resuscitation bay with a history of a syncopal episode. No family members or friends are present with the patient.
Case Summary
A 66-year-old female with a history of smoking, HTN and T2DM presents with syncope while walking her dog. She complains of retrosternal chest pain radiating to her jaw. She will become increasingly bradycardic and hypotensive, requiring the team to mobilize resources in order to facilitate diagnosis and management of an aortic dissection.
Download the case here: Aortic Dissection
First EKG for the case: 
(EKG Source: http://i0.wp.com/lifeinthefastlane.com/wp-content/uploads/2011/12/sinus-tachycardia.jpg)
Second EKG for the case:
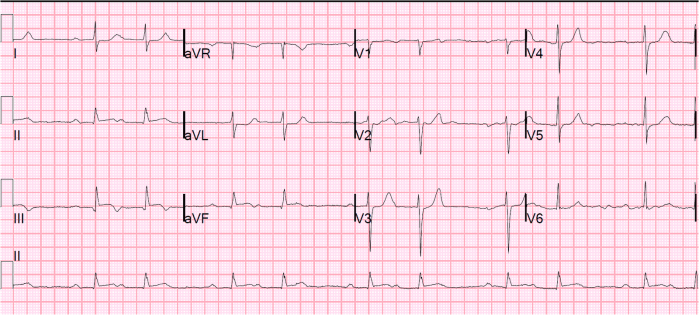
(EKG Source: http://hqmeded-ecg.blogspot.ca/2012_09_01_archive.html)
CXR for the case:

(CXR Source: https://radiopaedia.org/articles/aortic-dissection)

{kind=link}