This case was written by Dr. Martin Kuuskne from McGill University. Dr. Kuuskne is a PGY4 Emergency Medicine resident and one of the editors-in-chief at EMSimCases.
Why it Matters
Arrhythmogenic Right Ventricular Dysplasia (ARVD) is the second most common cause of sudden cardiac death in young people, after hypertrophic obstructive cardiomyopathy (HOCM). This case highlights three important aspects of the management of an arrhythmia in a young, previously healthy adult:
- The use of suitable antiarrhythmic agents in the setting of a stable, wide-complex tachycardia (WCT)
- The recognition of deterioration in a patient with a WCT and a pulse
- The difference between synchronized cardioversion and defibrillation and their respective indications during different ACLS algorithms
Clinical Vignette
You are working an evening shift in a community hospital emergency department. A 26-year-old man presents to the ED by ambulance after an episode of syncope while playing soccer.
Case Summary
A 26-year-old man who suffered a syncopal event while playing soccer presents to the emergency department with a stable wide-complex tachycardia (WCT). The patient must be treated with an antiarrhythmic medication or by synchronized cardioversion. The patient later deteriorates into an unstable WCT and then ventricular fibrillation requiring advanced cardiac life support (ACLS) and defibrillation.
Download the case here: ARVD Case
First ECG for case found here:

Second ECG for case found here:
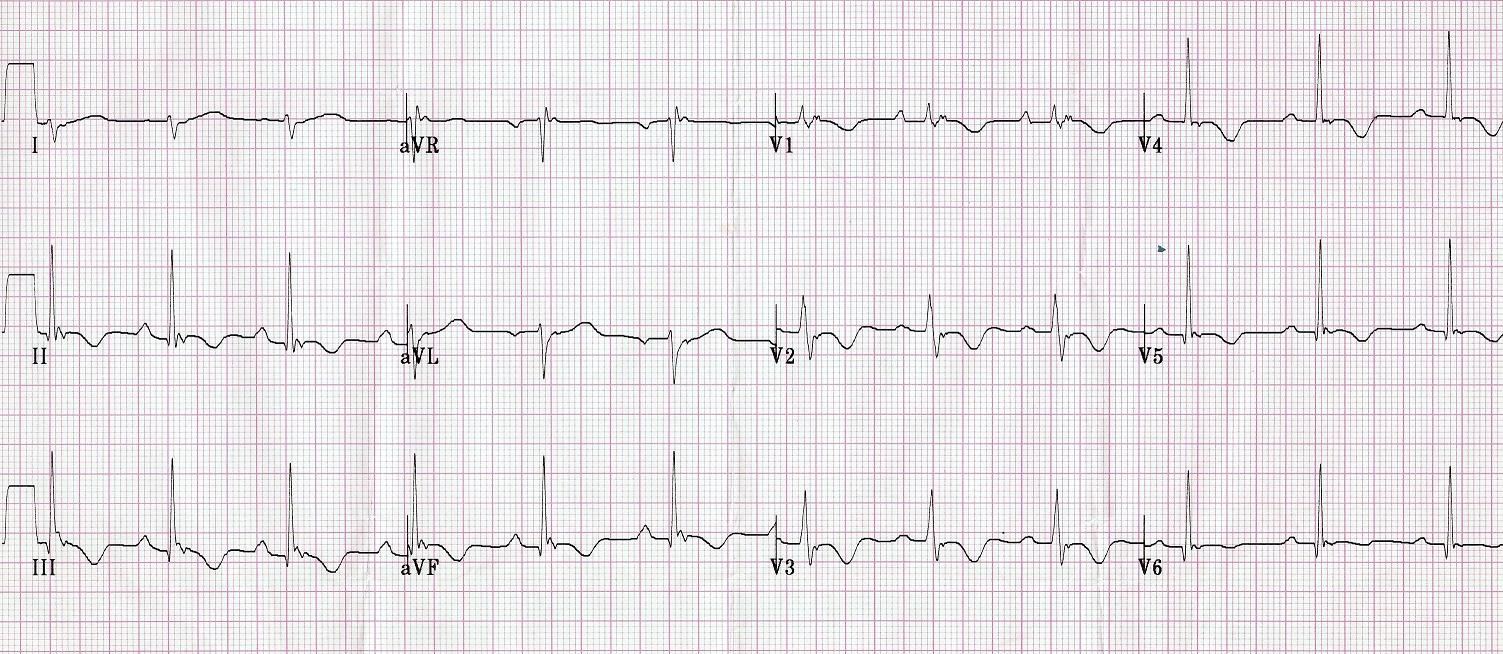
(ECG source: http://cdn.lifeinthefastlane.com/wp-content/uploads/2010/12/ECG-exigency-008_3.jpg)
CXR for case found here:

(CXR souce: http://radiopaedia.org/images/220869)

{kind=link}