This case is written by Drs. Quang Ngo and Donika Orlich. Dr. Ngo is an attending emergency physician at McMaster Children’s Hospital and also serves as the Associate Program Director for the Department of Pediatrics. He is also a member of the advisory board here at EMSimCases. Dr. Orlich is a PGY5 Emergency Medicine resident at McMaster University who also completed a fellowship in Simulation and Medical Education last year.
Why it Matters
Having an approach to the toxic neonate is essential. More importantly, emergency physicians must be able to recognize subtle historical clues and physical exam features that point toward congenital heart disease in order to begin critical treatment rapidly. This case highlights the following:
- The presentation of neonates with congenital heart disease including features like difficulty feeding, CHF, and tachypnea without increased work of breathing
- The clinical features that may be present in a coarctation of the aorta, one specific type of congenital heart disease, and the resultant need to include four-limb BP’s as part of the work-up of toxic-appearing neonates
- The importance of beginning a prostaglandin infusion in patients with suspected ductal-dependent congenital heart disease
- One of the most common side effects of a prostaglandin infusion – apnea
Clinical Vignette
Your triage nurse comes to tell you about an infant she just put in the resuscitation room who she feels looks quite unwell. He is a 2 week old neonate brought to the ED by his mother. Mom was worried because he hasn’t been feeding very well and seems to just get sleepy when feeding. Now he just vomited his last feed and seems really lethargic. She thinks he just “doesn’t look the right colour”.
Case Summary
A 2-week-old neonate presents in shock requiring the learner to implement an initial broad work-up. The patient will also be hypoglycemic, and will seize if this is not promptly recognized. Physical exam and CXR findings will suggest coarctation of the aorta as the likely cause, and the learner should recognize the need for gentle fluid boluses and a prostaglandin infusion. Unless learners anticipate appropriately and intubate the patient prior to beginning the prostaglandins, the infant will become apneic after starting the infusion and require intubation.
Download the case here: Coarctation of the Aorta Case
ECG for the case found here:

(ECG source: http://www.omjournal.org/IssueText.aspx?issId=380)
Initial CXR for the case found here:
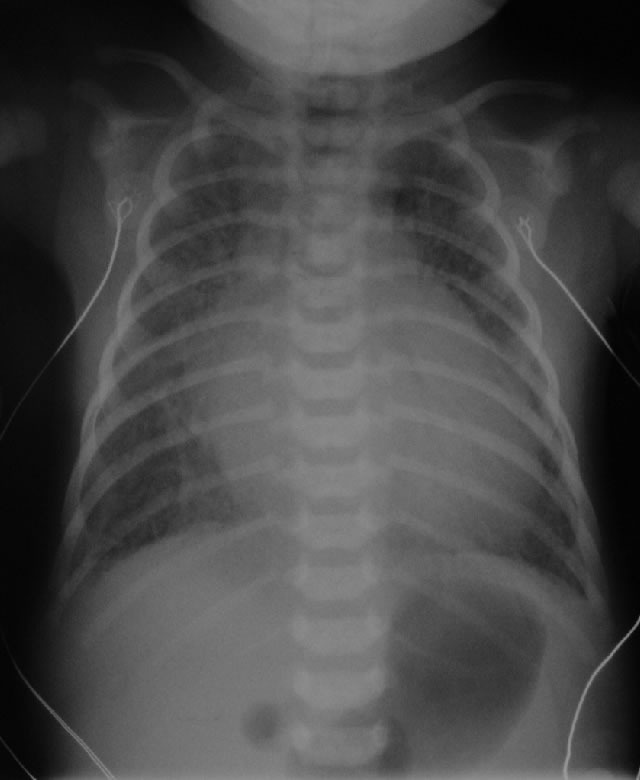
(CXR source: http://www.adhb.govt.nz/newborn/TeachingResources/Radiology/CXR/HLHS/CXR-HLHS-congested.jpg)
Post-intubation CXR for the case found here:
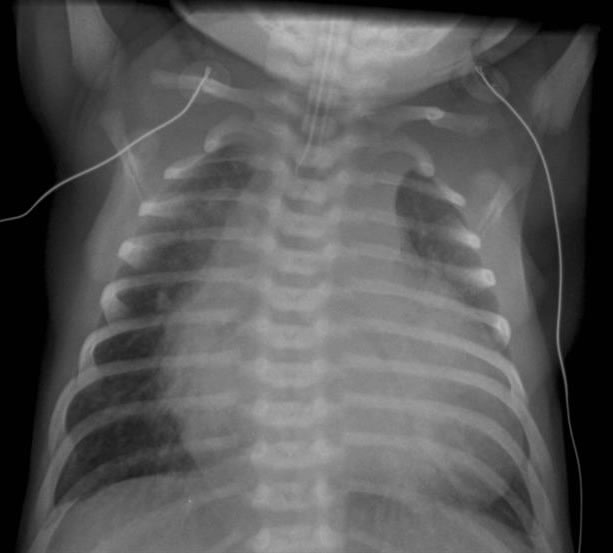
(CXR source: http://www.adhb.govt.nz/newborn/TeachingResources/Radiology/CXR/OtherCHF/NonstructuralCHF.jpg)
For more information on the management of Congenital Heart Disease Emergencies, see the excellent review by Emergency Medicine Cases found here.

{kind=link}
{kind=link}