This case is written by Dr. Kyla Caners. She is a staff emergency physician in Hamilton, Ontario and the Simulation Director of McMaster University’s FRCP-EM program. She is also one of the Editors-in-Chief here at EmSimCases.
Why it Matters
Calcium channel blocker overdoses are one of the most difficult overdoses for emergency physicians to manage. Even with excellent care, these patients often progress to cardiac arrest or to needing ECMO. This case highlights some key features in management, including:
- The use of calcium gluconate and high-d0se insulin infusions to assist with blood pressure support (in isolation or in addition to other vasopressors)
- The use of intralipid as an end of the line rescue treatment
- The need to consider co-ingestions and their effects on management (in this case, clonazepam that slows the patient’s respiratory rate enough to require intubation)
Clinical Vigenette
A 48-year-old female presents to the ED with an unknown overdose. She was out drinking with friends until an hour ago. Her daughter came home and found her with vomit around her, empty pill bottles, and bits of pills in her vomit.
Case Summary
A 48-year-old female presents with a possible multi-drug overdose including glyburide, clonazepam and nifedipine. She will remain hypotensive throughout the case, despite treatment with calcium, high dose insulin, and other vasopressors. She will also have progressive respiratory depression and will eventually require intubation. She will then proceed to arrest. The team will be expected to give intralipid once the patient has arrested.
Download the case here: Multi-drug (CCB) OD
ECG for the case found here:
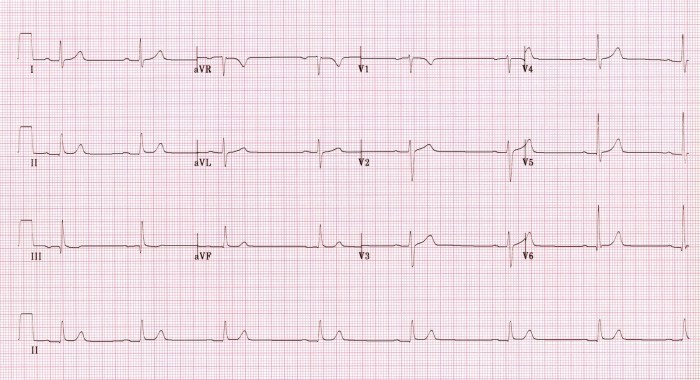
(ECG source: http://lifeinthefastlane.com/ecg-library/beta-blocker-and-calcium-channel-blocker-toxicity/sb-1hb/)
Post-intubation CXR for the case found here:
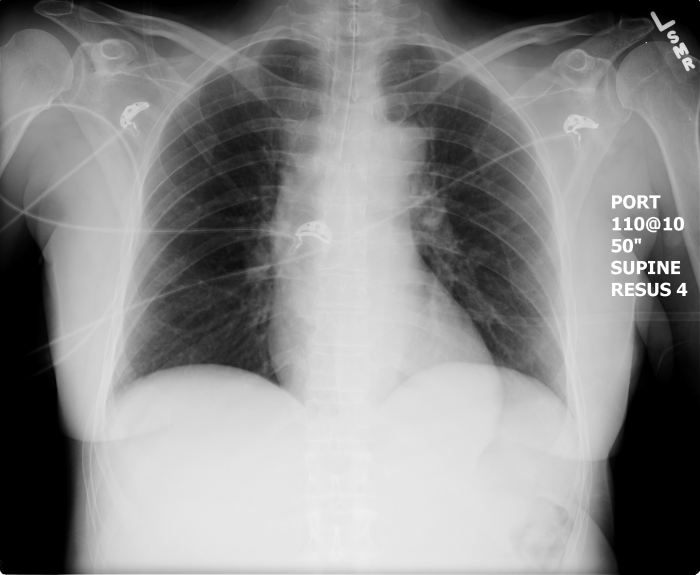
(CXR source: https://emcow.files.wordpress.com/2012/11/normal-intubation2.jpg)

{kind=link}