This is the fourth in a case series we will be publishing that make up “The Nightmares Course”.
The Nightmares Course at Queen’s University (Kingston, Ontario) was developed in 2011 by Drs. Dan Howes and Mike O’Connor. The course emerged organically in response to requests from first year residents wanting more training in the response to acutely unwell patients. In 2014, Dr. Tim Chaplin took over as the course director and has expanded the course to include first year residents from 14 programs and to provide both formative feedback and summative assessment. The course involves 4 sessions between August and November and a summative OSCE in December. Each session involves 4-5 residents and covers 3 simulated scenarios that are based on common calls to the floor. The course has been adapted for use at the University of Saskatchewan, the University of Manitoba, and the University of Calgary.
Why it Matters
The first few months of residency can be a stressful time with long nights on call and the adjustment to a new level of responsibility. While help should always be available, the first few minutes of managing a decompensating patient is something all junior residents must be competent at. This case series will help to accomplish that through simulation.
Clinical Vignette
It’s 1:00 AM and you’ve been called to assess a 69 year old woman admitted to the Gyne Oncology unit. She was recently diagnosed with ovarian cancer and is actively receiving chemotherapy. Her repeat CT showed decreased tumor burden and the plan is for surgery tomorrow. She was admitted pre-op to receive a blood transfusion for a Hb of 72. The transfusion ended 4 hours ago and was tolerated well. Approximately 30 min ago, the patient started developing shortness of breath and central chest discomfort.
Case Summary
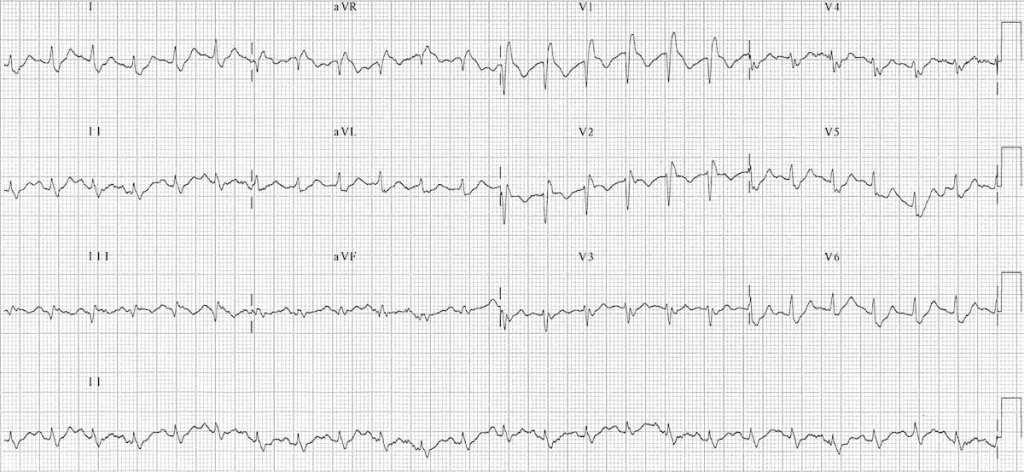
This case involves the approach to the patient with acute dyspnea. The patient is tachypneic but with an otherwise normal respiratory exam. ECG shows new right heart strain. The team should consider multiple possibilities but recognize PE as the most likely cause.
The team is expected to appropriately call for help while initiating management. The patient will decompensate and arrest – thrombolytics should be discussed. After the patient achieves ROSC, the resident will provide handover to the code blue team.
Download here
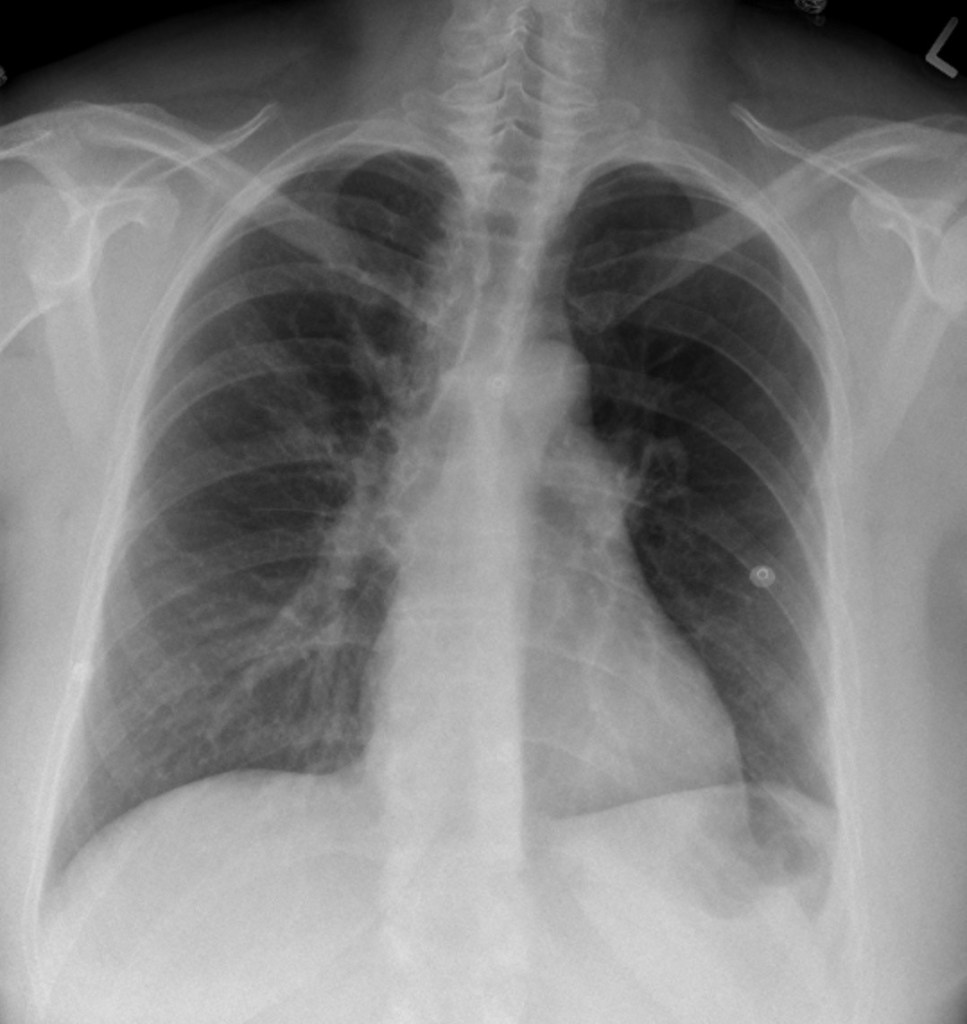
Chest X-ray for the Case
EKG for the Case