This is the twelfth and final case in a series we are publishing that make up “The Nightmares Course” – a Sim Bootcamp for new residents.
The Nightmares Course at Queen’s University (Kingston, Ontario) was developed in 2011 by Drs. Dan Howes and Mike O’Connor. The course emerged organically in response to requests from first year residents wanting more training in the response to acutely unwell patients. In 2014, Dr. Tim Chaplin took over as the course director and has expanded the course to include first year residents from 14 programs and to provide both formative feedback and summative assessment. The course involves 4 sessions between August and November and a summative OSCE in December. Each session involves 4-5 residents and covers 3 simulated scenarios that are based on common calls to the floor. The course has been adapted for use at the University of Saskatchewan, the University of Manitoba, and the University of Calgary.
Why it Matters
The first few months of residency can be a stressful time with long nights on call and the adjustment to a new level of responsibility. While help should always be available, the first few minutes of managing a decompensating patient is something all junior residents must be competent at. This case series will help to accomplish that through simulation.
Clinical Vignette
It is 3:00 am, you are called to the floor to assess a 73-year old man, Mr. Brown, who was admitted to general surgery 2 days ago, and has a scheduled large bowel resection for diverticulitis tomorrow. He has been undergoing bowel prep.
You are called because he is experiencing confusion, shortness of breath, and chest heaviness.
CASE SUMMARY
This case involves the assessment and management of an acutely confused patient with hypertensive encephalopathy. The resident is expected to initiate appropriate supportive measures (ensure working IV, oxygen, monitors) while obtaining a focused history and performing a focused physical exam, including a detailed neurologic assessment. They should recognize the elevated blood pressure and order a work-up for end-organ damage. The patient will require transfer to a critical care setting for administration of acute blood pressure lowering agents including involvement of RACE or a similar high acuity response team.
DOWNLOAD HERE – NIGHTMARES 12: HTN Encephalopathy
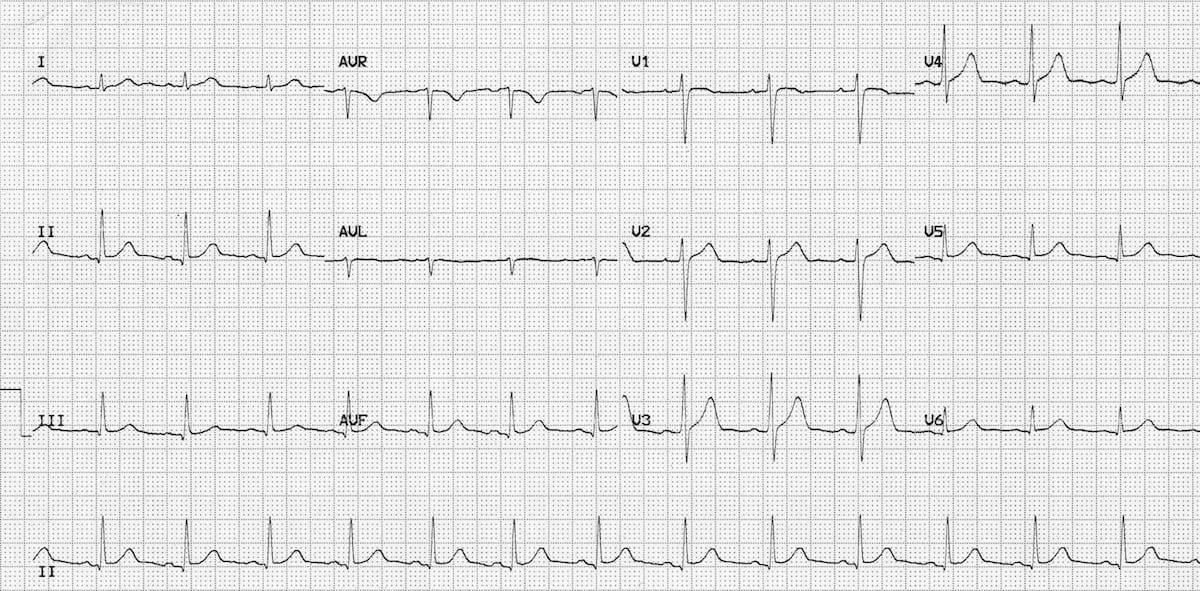
EKG FOR THE CASE