This case was written by Drs. Pittman and Bridges, emergency physicians at Prisma Health-Upstate in Greenville, SC. They both teach in the University of South Carolina School of Medicine-Greenville and in the emergency medicine residency program.
Dr. Pittman is the residency Director of Academic Success, completed residency at the Georgetown / Washington Hospital Center Emergency Medicine Residency and medical school at the University of Virginia School of Medicine. He is interested in resident and student education, wilderness medicine, and psychology. He completed the ACEP Teaching Fellowship and is a Fellow of the Academy of Wilderness Medicine.
Dr. Bridges is the Assistant Clerkship Director in Emergency Medicine. She completed residency at the Medical University of South Carolina and medical school at the University of North Carolina at Chapel Hill. She is interested in resident and student education, developing residents as teachers, and medical education. She is active in the South Carolina Chapter of the American College of Emergency Physicians.
Why It Matters
Managing unstable patients is the specialty of emergency physicians and training for this needs to start early. But these patients are relatively rare in clinical practice and it can be difficult for junior learners to get a fulsome learning experience at the bedside. By exposing junior learners to unstable patients in the safety of the sim lab, they can fine tune their knowledge of important algorithms and practice the leadership and decisive action that are necessary for high quality clinical care. Knowledge and crisis resource management (CRM) gaps can be identified and improved without putting patient safety at risk.
Clinical Vignette
While eating breakfast this morning, our patient had a sudden onset of feeling like his heart was racing. He then developed shortness of breath, which has not improved. EMS was called by family when he got lightheaded standing up from the table. He is mildly confused and mentions mild chest discomfort.
Case Summary
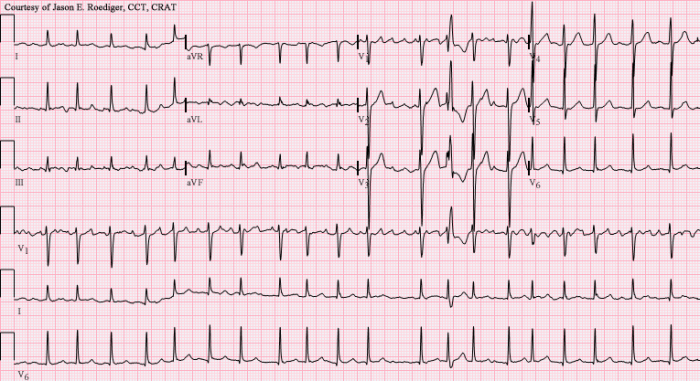
A 72-year-old male presents with sudden onset palpitations and shortness of breath and is found to be in unstable atrial fibrillation with RVR. In the ED he is hypotensive with an altered level of consciousness and requires emergent cardioversion.
Download the case here: Unstable AFib