What is it?
Realism is the degree to which your simulation environment recreates or mimics the patient environment for your learners.
A word on fidelity.
The terms realism and fidelity are essentially interchangeable. However, many often associate the term fidelity with the amount of technology used to recreate the patient environment. For example, when educators refer to a case as “high fidelity” what they often mean is that they are using a costly computer-based mannequin with all the bells and whistles. The caveat, of course, is that having cutting edge equipment does not, on its own, ensure that the learner’s experience approaches reality. I prefer the term realism because it reminds us that there are more things to simulate than just the physical environment.
Why it’s important.
The basic premise of simulation as an educational modality is that it allows direct observation of a learner’s behaviour. Furthermore, debriefing in simulation allows discussion about noted learner deficiencies. Teasing out the learner’s cognitive process and knowledge gaps to discover the origins of the learner’s behaviour is paramount. In order to elicit true behaviour from a learner, (i.e. – behaviour that most closely mirrors their performance with real patients) the learner must treat the situation as a real one. And to do so, they must believe in it.
If the environment in which the learner is practising does not even come close to imitating reality, then the learner will not fully engage in the learning exercise. This limits the ability of the instructor to assess the learner’s abilities. In addition, not addressing realism lets learners use it as an excuse for their performance. For example, “If the mannequin had better breath sounds, I would have decompressed the tension pneumothorax.” Or “If this case was in the Emergency Department, I’m sure I would have seen the VT on the monitor and then shocked the patient.”
Making the environment mirror reality does not necessarily require high tech equipment. It does, however, require engaging the learners and addressing limitations to realism before the scenario begins. Orient learners to the mannequin so they know where they can feel pulses and where to listen for breath sounds. If the mannequin doesn’t have these things, let the learners know how to ask for physical exam findings. It is remarkable how well learners can engage in a scenario with a mannequin that has no high tech functions. They are only able to do this if you create conceptual realism.
Types of realism
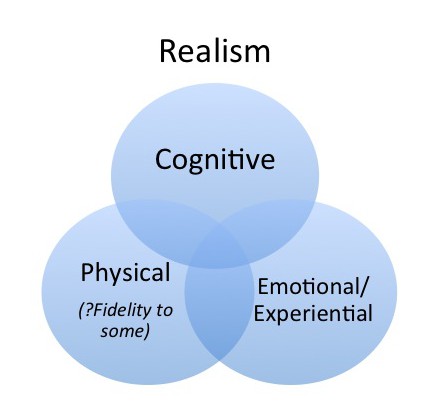
In 2007, Rudolph, Simon, and Raemer described three different types of realism as essential to simulation training.1 Their terminology was a slight modification of Dieckmann’s work on the aspects of realism, also published in 2007. 2 The three components of realism highlighted by Rudolph et al are as follows:
1) Conceptual
Conceptual realism allows learners to think about a case in the same manner they would for a real patient. The most important component to creating conceptual realism is providing the learners with enough information to accurately frame the case. For example, you would expect a patient with a tension pneumothorax to have tachycardia, hypotension, and decreased breath sounds on one side. How this information is conveyed matters less than the fact that the information is logical in the context of the case.
To understand the power of conceptual realism, look to oral exams. The learner is able to make a diagnosis and manage a patient without any physical cues present. Oral exams can create conceptual realism. Conceptual realism is crucial to a good simulation scenario. And sometimes, adding too many bells and whistles actually takes away from the concept.
Yes, that’s right. You can be very low tech and still run fantastic simulation. You just need to set the stage, meet minimum cognitive standards, and debrief.
2) Physical
There are some things that just need to be practised in real time and space. Physical realism is most important for procedural skills. Practising airway management on an airway head that has unrealistic anatomy just doesn’t help learners to develop the motor memory they need. This doesn’t mean that all simulators need to be exact replicas. But to create physical realism, a task trainer must emulate the necessary motor feedback required to practise a skill properly. For example, a chest tube trainer doesn’t need to be an entire pig chest. It does, however, need to have an appropriate degree of resistance so that learners develop the sense of how hard to push in order to penetrate the pleura.
All mannequins have poor physical realism in some way. But with enough cognitive and experiential realism, it doesn’t need to affect the quality of the learning experience.
3) Emotional and experiential
This is the type of realism that puts a knot in your stomach. Experiential realism is about creating the emotions that often make our jobs difficult. Examples would include having a mother sob in the corner while trying to run a code on her infant child. Or having a difficult parent present who becomes obtrusive to care. Or how horrifying it can be to see a patient with a GI bleed exsanguinating from their mouth. Perhaps the challenge is creating the cognitive burden that goes along with managing two patients at once. Or perhaps the experiential realism comes from the frustration of dealing with a team that is obviously ignoring your direction. In other words, experiential realism is important to consider if the purpose of a case is to practice working through an emotionally challenging case or to teach techniques for overcoming a difficult family member or team member. It is also an important part of why junior learners can find simulation intimidating – because good experiential realism recreates the fear or discomfort that goes with being uncertain how to manage a particular condition. Again, your mannequin can be a cabbage patch kid doll if your sobbing parent actor is good enough.
The reality of realism
Realism is essential to simulation. As a simulation educator, you should be aware of which aspects of realism are most important for the case you are designing. Do you need to create an appropriate cognitive environment to assess the resident’s management of a TCA overdose? Do you need to see how the resident can lead a difficult team? Or do you need to see that a resident can skilfully perform a cricothyroidotomy? Or do you need all three components to assess a resident’s management of a pediatric trauma? Design your case and supplies with your realism goals in mind.
References
- Rudolph JW, Simon R, Raemer DB. Which reality matters? Questions on the path to high engagement in healthcare simulation. Simul Healthc. 2007;2(3):161-163. doi:10.1097/SIH.0b013e31813d1035.
- Dieckmann P, Gaba D, Rall M. Deepening the theoretical foundations of patient simulation as social practice. Simul Healthc. 2007;2(3):183-193. doi:10.1097/SIH.0b013e3180f637f5.
