Note: This case has been updated to reflect the ACLS 2020 Guidelines.
Download the case here: VSA Megacode (ACLS 2020 Update)
This case is written by Dr. Cheryl ffrench, a staff Emergency Physician at the Health Sciences Centre in Winnipeg. She is the Associate Program Director and the Director of Simulation for the University of Manitoba’s FRCP-EM residency program; she is also on the Advisory Board of emsimcases.com.
Why it Matters
Leading a resuscitation is a core skill of an Emergency Physician. More often than not, we know very little about the patient’s history before orchestrating a team of nurses, respiratory technicians, residents and other team members to provide resuscitative care. Assessment of the cardiac rhythm and pulse allows us to start with ACLS algorithms in order to hopefully obtain return of spontaneous circulation (ROSC), initiate post-ROSC care and arrange for the appropriate disposition of the patient This case, which is geared toward junior learners, highlights the following:
- The importance of resource allocation during a prolonged resuscitation
- Managing the resuscitation team, ensuring effective communication and recognizing compression fatigue.
- Providing high quality ACLS and post-ROSC care
- Recognizing STEMI as the cause of the cardiac arrest and initiating disposition for percutaneous coronary intervention (PCI)
Clinical Vignette
A 54-year-old male police officer presents to the ED with chest pain. He played his normal weekend hockey game about two hours ago. He has been having retrosternal chest pain since the game ended. It improved with rest, but has not resolved completely. It is worse after walking into the department. He now feels dizzy, short of breath, and nauseous.
Case Summary
A 54-year-old male police officer presents to the ED complaining of chest pain for two hours that started after his weekend hockey game. He is feeling dizzy and short of breath upon presentation. He will have a VT arrest as he is placed on the monitor. He will require two shocks and rounds of CPR before he has ROSC. He will then loose his pulse again while the team is trying to initiate post-arrest care; this will happen several times. Finally, the team will maintain ROSC. When an ECG is performed, it is revealed that the patient has a STEMI and the team will need to call for emergent PCI.
Download the case here: VSA Megacode
ECG for the case found here:
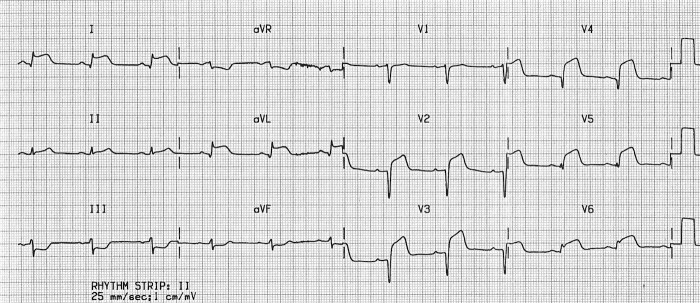
| (ECG source: http://cdn.lifeinthefastlane.com/wp-content/uploads/2011/10/anterolateral.jpg) |
Post Intubation-CXR for the case found here:
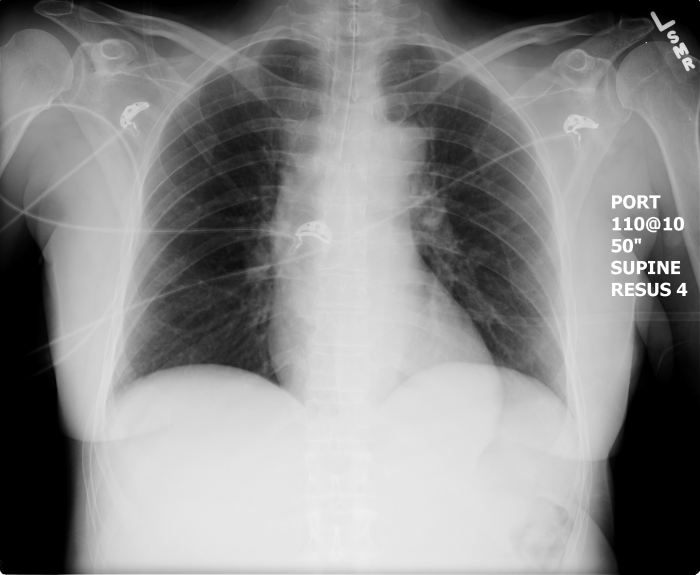
| (CXR source: https://emcow.files.wordpress.com/2012/11/normal-intubation2.jpg) |

{kind=link}
{kind=link}
One thought on “VSA Megacode”