This case is written by Drs. Nicole Kester-Green and Jen Riley. Dr. Kester-Greene is a staff physician at Sunnybrook Health Sciences Centre in the Department of Emergency Services and an assistant professor in the Department of Medicine, Division of Emergency Medicine. She has completed a simulation educators training course at Harvard Centre for Medical Simulation and is currently Director of Emergency Medicine Simulation at Sunnybrook. Dr. Riley is a staff emergency physician at St. Michael’s Hospital and assistant professor at the University of Toronto. Her areas of interest are in simulation and medical technology, with a focus on developing programs and curriculum for trainees and faculty both in medicine and allied health professions.
Why it Matters
Patients who present to the ED with agitation can be very challenging to manage. It is particularly difficult when the patient clearly lacks capacity and is unable to respond appropriately to any simple commands. In these situations, ensuring the safety of both the patient and staff members becomes the primary goal. This case highlights, specifically:
- That chemical restraint should always be used if physical restraints are to be used
- The challenges to assessing a patient who is clearly unwell when that patient is not cooperative
- The role security plays in ensuring a safe patient care experience
A Note on Safety
Pre-briefing is always an important component of simulation. For this case, it is essential that the pre-briefing takes a little extra time so that the safety of everyone involved is reviewed. The case is designed so that physical restraints are only placed once the standardized patient is traded for a mannequin. Regardless, both the standardized patient and the sim participants should be briefed on the use of simulated restraint. It is essential that a safe word like “time out” is pre-determined in case any participants are feeling unsafe at any point in the case. This would immediately halt the case. Similarly, instructors must be watching closely for safety and cut the scenario if they feel anyone may be harmed. We advocate for having security participate in this case as learners. However, briefing security that they should not use the restraints on the standardized patient would also help ensure safety.
Clinical Vignette
The charge nurse comes to you: “There is a 68 year old woman in the seclusion room. She was observed pacing and acting bizarre at the bus stop. EMS managed to talk her into ambulance. On route she told them her neighbour is trying to poison her. Initially, she was calm but now she is starting to get agitated. She doesn’t have any previous psych admissions in the system. We couldn’t get any vital signs.
Case Summary
A 68-year old woman is found at a bus stop exhibiting bizarre behaviour. She is brought to the ED by paramedics. In the ED, she is expressing paranoid delusions. Her agitation escalates and does not respond to verbal de-escalation or an overwhelming show of force. She will require physical and chemical sedation to facilitate the work-up for her new onset psychosis.
Download the case here: Elderly psychosis and agitation
ECG for the case found here:
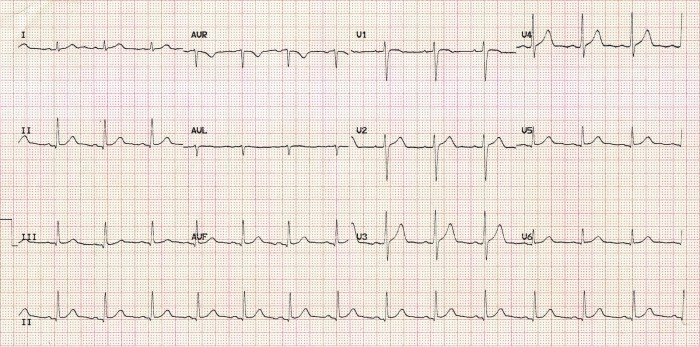
(ECG source: https://lifeinthefastlane.com/ecg-library/normal-sinus-rhythm/)
