This week’s case is written by Drs. Ashley Lubberdink and Sameer Sharif. Dr. Lubberdink is a PGY4 Emergency Medicine resident at McMaster University and is just beginning her fellowship in simulation and medical education. Dr. Sharif is a PGY5 Emergency Medicine resident at McMaster University who has just completed his fellowship in simulation and medical education.
Why it Matters
LVADs are pretty uncommon devices! If your practice location is not a hospital that inserts LVADs, then it is likely that you have never come across a patient with an LVAD. Without prior knowledge of these devices, it can be quite distressing trying to assess these patients. This case is designing to highlight the following:
- LVAD patients do not have a pulse, a measurable blood pressure, or a detectable heart rate on the sat probe
- To assess for blood pressure, one must insert an arterial line or use a blood pressure cuff and doppler U/S to obtain the MAP
- Early after LVAD placement, drive line infection and bleeding are common complications
- Call for help early! These patients generally have care providers who are available to help trouble shoot by phone at all hours of the day
More Reading
For more information on an approach to LVADs, we suggest the following sources:
https://emcrit.org/emcrit/left-ventricular-assist-devices-lvads-2/
https://canadiem.org/lvads-approach-ed/
Clinical Vignette
A 62-year-old male presents to your large community ED with a 1 day history of generalized malaise and nausea and a 2-hour history of palpitations. He is particularly concerned about his symptoms because last month he had an LVAD placed at your provinces’ major cardiac center (3 hours away) for stage 4 CHF. His wife is accompanying him but is currently parking the car.
Case Summary
A 62-year-old man presents to the ED with palpitations and general malaise. On initial assessment, the team finds out he had an LVAD placed within the last 1 month. The team will need to work through how to assess the patient’s vital signs appropriately and will discover the patient has a low MAP and a low-grade fever. On inspection, the patient’s drive line site will appear infected. The initial ECG will show features of hyperkalemia. After the initial assessment, the patient will progress to a PEA arrest requiring resuscitation by ACLS protocols. Labs will reveal an acute kidney injury and hyperkalemia. The patient will obtain ROSC when the hyperkalemia is treated.
Download the case here: LVAD Case
Initial ECG for the case found here:
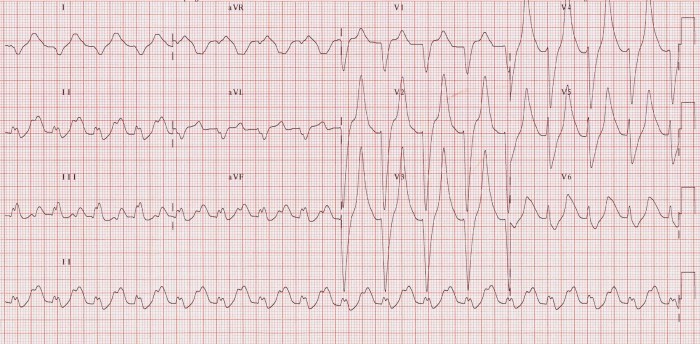
(ECG source: https://lifeinthefastlane.com/ecg-library/basics/hyperkalaemia/)
Second ECG for the case found here:
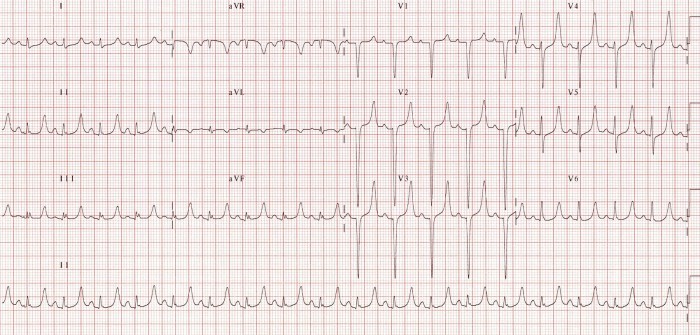
(ECG source: https://lifeinthefastlane.com/ecg-library/basics/hyperkalaemia/)
CXR for the case found here:
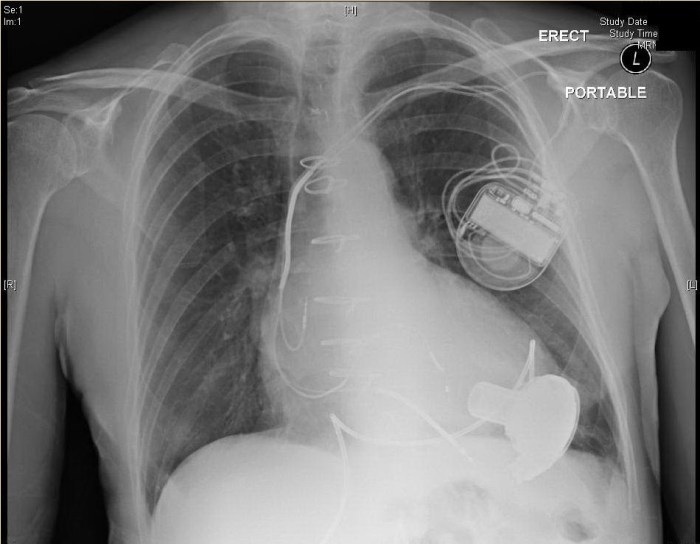
(CXR source: https://edecmo.org/additional-technologies/ventricular-assist-devices-vads/lvads/)
Picture of drive line site infection found here:

(Picture source: http://journals.sagepub.com/doi/full/10.1177/1179065217714216)
Echo for case found here:
(Echo source: https://www.youtube.com/watch?v=-4ThAo4m2UI)
