This case was written by Dr. Larissa Hattin.
Dr. Hattin is a current PGY5 Emergency Medicine Resident at University of British Columbia- Victoria site. She has always been interested in medical education and this year completed a postgraduate certificate program at Oxford University in teaching evidence-based medicine. She completed her BSc with Honours at Guelph University and her MD from McMaster University. Her other interests include physician leadership, curriculum design and surfing!
WHY IT MATTERS
Undifferentiated abdominal pain is one of the most common presentations in the ED. Frequently we have to make decisions quickly with limited information. This case highlights that tension between stabilizing the patient and trying to find out what is going on in the setting of limited historical details.
CLINICAL VIGNETTE
67M with multiple comorbidities, here today with 3 days of gradually worsening abdo pain. Vomited twice at home. Hx of ETOH. Brought by EMS.
CASE SUMMARY
A 67yr old male with multiple comorbidities is brought by ambulance with a 3-day history of diffuse abdominal pain. The history is vague and the differential of his symptoms remains very broad. He develops significantly worsening pain and hypotension and becomes obtunded. As the patient’s condition deteriorates, the team must initiate management of abdominal pain plus shock and support the hemodynamics with vasopressors/inotropes. The team will need to intubate to facilitate advanced imaging and definitive care.
DOWNLOAD THE CASE HERE:
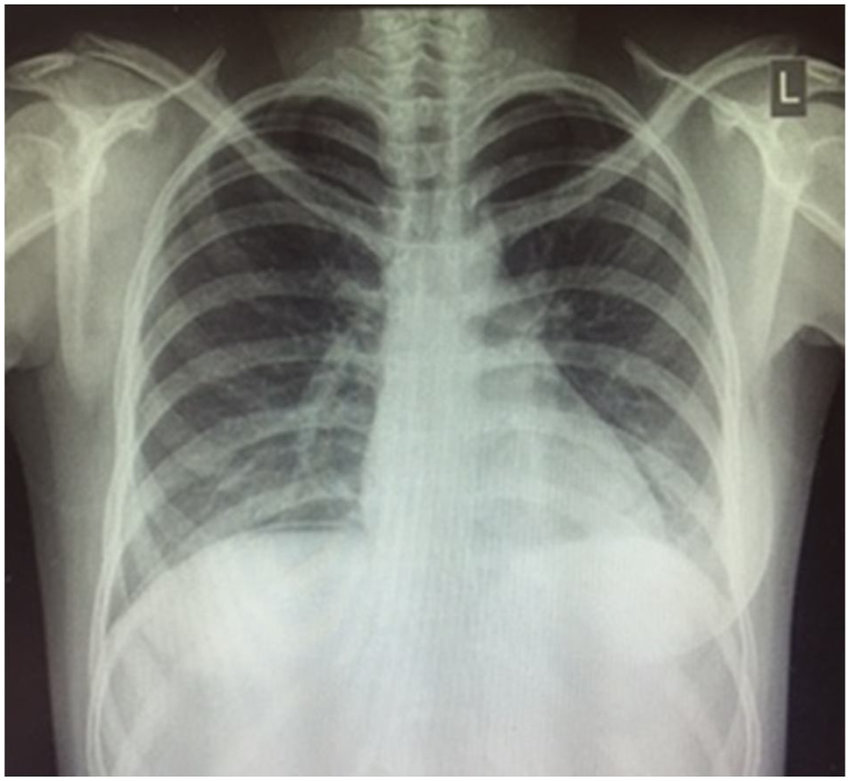
Image courtesy of https://www.researchgate.net/figure/Erect-chest-x-ray-demonstrating-subdiaphragmatic-free-air_fig1_323084315
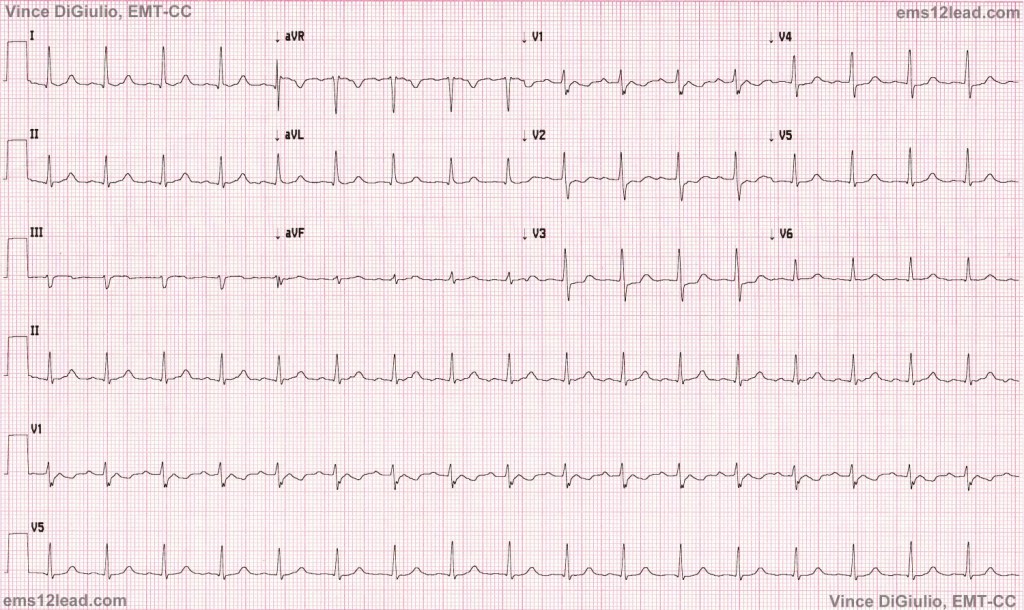
ECG Courtesy of http://ems12lead.com/2015/12/26/12-rhythms-of-christmas-sinus-tach/

{kind=link}